



“The real concern with diagnoses of Irlen Syndrome is that it can distract from genuine diagnosis and treatment, such as a comprehensive evaluation by an educational psychologist followed by the appropriate remedial educational input,” said RANZCO spokesperson Professor Frank Martin, a Sydney-based paediatric ophthalmology and strabismus specialist. “Any interventions that distract from and delay this evaluation could be detrimental to the effective treatment of any learning disabilities.”
RANZCO’s position statement and supporting Q&A
What claims have been made to support the existence of Irlen Syndrome?
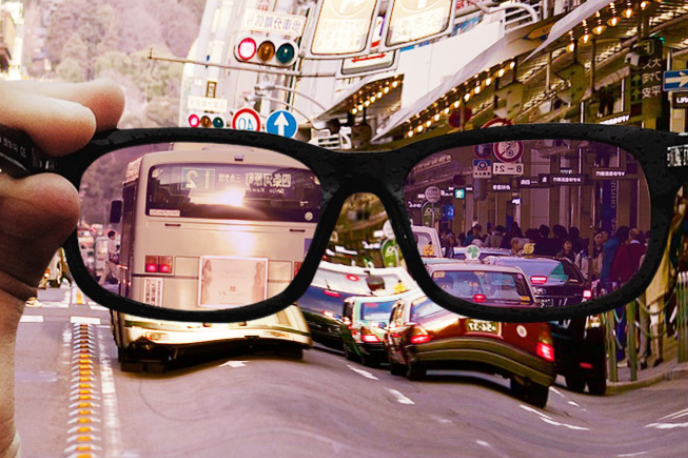
Irlen Syndrome was defined by Helen Irlen in 1983 as a perceptual processing disorder, specifically that the brain is unable to properly process visual information transmitted from the eye because of sensitivity to certain wavelengths of light¹. This is said to lead to “visual stress” and “distortions” which result in diverse symptoms such as poor concentration, difficulties with reading, writing and comprehension, glare sensitivity, headaches and poor depth perception². Irlen Syndrome is also known as Scotopic Sensitivity Syndrome or Meares-Irlen Syndrome.
What claims are made when reporting the prevalence of Irlen Syndrome?
Prevalence rates differ widely in the literature and this is, at least partly, due to the criteria which requires individuals (often children) to self-report their symptoms. Irlen reports 46% of children with reading problems as being affected by Scotopic Sensitivity Syndrome². Other proponents of Irlen Syndrome quote that 12-15% of the general population is affected, and 45% of those with learning difficulties⁴.
How is it purported that Irlen Syndrome be assessed and treated?
Individuals complete a subjective assessment including a questionnaire to ascertain the level of “visual stress”. They are then asked to complete tasks intended to create this visual dysfunction. The individual is subsequently re-tested but with coloured overlays or tinted lenses, whilst noting any apparent improvement in symptoms, comfort levels and reading fluency. A prescription for coloured overlays or lenses (coloured filters) is generated based on this information.
What claims are made to support the rationale for the treatment of Irlen Syndrome?
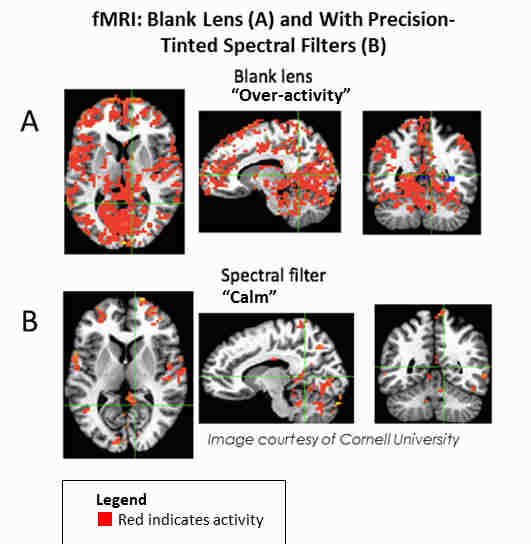
The Irlen method claims that coloured filters improve the brain’s ability to process visual information by filtering out particular light waves, leading to more fluent and comfortable reading and restoring the visual pathway back to “normal”⁴.
Plausibility of Irlen Syndrome as a condition
1. Lack of scientific evidence that Irlen Syndrome exists as an entity
Despite Irlen Syndrome being first described in the early 1980’s there is still no sound theoretical basis or evidence that the condition actually exists. A diagnosis of Irlen Syndrome is based solely on symptoms with no quantitative physiological correlation. There remains a lack of clearly established criteria. In fact, the only defining criterion is a self-reported benefit of coloured filters while reading³. While the premise is “scotopic” sensitivity, it is the photopic system that is used for reading⁵. Importantly, those with Irlen Syndrome do not show any electrophysiological changes of retinal function compared to control groups⁶,⁷. There is also a large disparity in prevalence rates which suggests a fundamental problem in definition⁸.
2. Lack of evidence that treatment for Irlen Syndrome is effective
Consistently, systematic and critical reviews have shown no scientific basis for the benefit of tinted lenses in reading disorders³, ⁸-¹⁴. There are no objective quantitative measurements available to assess or monitor treatment. The studies that have purported to show some benefit have generally suffered from poor methodology, selection bias, small sample numbers and lack of control groups. Often these are individual reports or testimonials, interviews or anecdotal evidence³, ⁹, ¹³.
3. Issues with lens choice
(a) Each individual is required to indicate their preference for coloured overlay/lenses. Not surprisingly a gender-based preference is often apparent with girls generally choosing pink or purple tints whereas boys generally choose blue tints¹⁴.
(b) Poor repeatability of colour choices – proponents of Irlen Syndrome and visual stress claim that a very precise colour is needed and highly specific to the individual, which only they are able to provide. Furthermore, they claim that the use of an incorrect colour would actually worsen the individual’s symptoms. It would therefore follow that there would be high repeatability in colour choice, but recent studies have shown poor inter-test consistency and repeatability³,¹⁴.
4. Issues with self-reporting
There are obvious problems inherent in any practice which relies solely on a population to self-report their symptoms and/or respond to leading questions, and this is particularly so in children. Symptoms of Irlen Syndrome are vague, non-specific and can be highly variable from day-to-day depending on external factors such as tiredness or illness. In addition, they frequently overlap with known ocular disorders eg. convergence insufficiency, accommodation difficulties or refractive errors.
Why do parents claim to see great improvement in their child’s reading with Irlen lenses?
There are several reasons why this may appear to be the case:
1. Placebo effect
Believing the lenses will help may give the impression of improvement. However, studies have shown improvements in reading with coloured overlays and lenses are no greater than in control groups³,⁷,⁹-¹²
2. Performance bias (Hawthorne effect)
A person who realises that they are being observed or tested tends to change their behaviour to perform at their best
3. Increased attention
A parent showing more interest and spending more time reading with a child is likely to have a beneficial effect on the child’s level of reading
4. Concurrent remedial programme
Many children are also in reading assistance programmes which are likely to improve reading
5. Natural development
Improvement in reading is a natural consequence of development and maturation. A child’s reading ability is likely to improve with age and practice regardless of whether Irlen lenses are used.
What is the verdict?
Due to a critical lack of scientific evidence that Irlen Syndrome exists or that treatment methods do anything to improve an individual’s performance, RANZCO cannot endorse treatment of the condition. This is in accordance with a joint statement issued in 1984, and reaffirmed in 2014, by the American Academy of Ophthalmology, the American Academy of Paediatrics, the American Association for Paediatric Ophthalmology and Strabismus and the American Association of Certified Orthoptists.
See other articles in this feature:
References