


A clear view of the ciliary zonule, or zonule of Zinn, is an uncommon sight at the slit lamp. Being transparent, poorly preserved post-mortem and resistant to absorbing histological stains, it wasn’t until the end of the 19th century that consensus on its anatomy was achieved. A recent comprehensive review by Bassnett (2021) summarises the important anatomical and physiological details of the zonule1. Here, we present clinical images of two uncommon conditions that highlight zonule insertion into the crystalline lens.
The zonular fibres arise in the bays of the pars plana and travel parallel to this structure towards the ciliary body. They arise as fine fibres that come together to their final thickness as they enter the valleys between the ciliary processes. They deviate course here to approach the lens and attach into a 1.5mm-wide area encircling the lens equator1. The majority attaches to the anterior and, to a slightly lesser extent, the posterior surface of this zone, while a minority attach nearer the equator.
A zonular fibre consists of a number of approximately 1-2μm-diameter bundles comprised of hundreds or thousands of individual microfibrils. The backbone of each microfibril is a fibrillin polymer with a glycan coat, 10-12nm in diameter and of indeterminate length1. These zonules are derived from cells of the non-pigmented ciliary epithelium but are also probably contributed to by the lens and other anterior segment tissues.
Zonule functionality
The zonule of Zinn has three main functions. Firstly, these fibres centre and hold the lens in anatomical position (circumferential suspensory ligament) under a degree of tension. When the ciliary muscle contracts, tension increases in the fibres over the pars plana and reduces in those attaching to the lens. This allows for accommodation as reducing zonular tension causes the lens to become more spherical, increasing its refractive power. When the ciliary muscle relaxes, the tension in the zonular fibres over the pars plana returns the crystalline lens to its distance vision state, sometimes termed dis-accommodation1. It has also been postulated that the zonule may also have a role in lens size and shape.
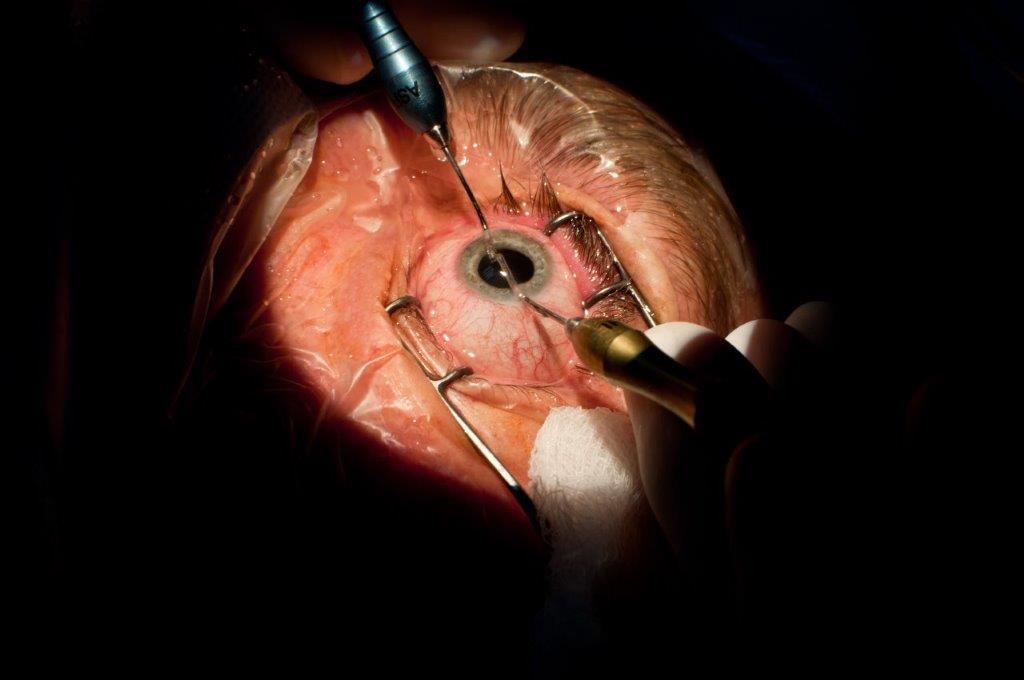
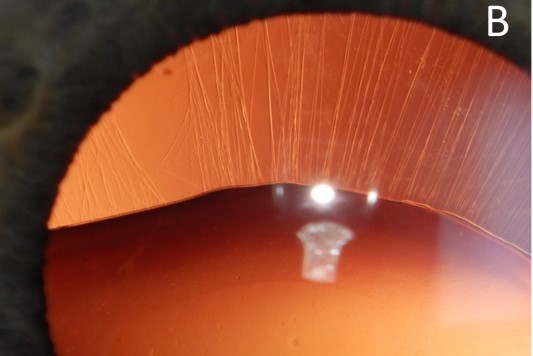
Normally the zonules of Zinn are hidden from view behind the iris, although elements of the anteriorly inserted zonules can sometimes be seen following maximum pharmacologic pupillary dilation. Therefore, due to the unusual circumstance of a) a sector iridectomy for an inferior iris tumour and b) significant crystalline lens luxation, the accompanying anterior segment photographs showcase the zonules attaching to the lens capsule in a clinical setting. In Fig A, the healthy, normal, high-density zonules are exposed secondary to an inferior iridectomy. In Fig B, elongated zonules with lower density and areas of absence highlight ectopia lentis secondary to zonular insufficiency.

Fig A. Healthy, normal, high-density zonules are exposed secondary to an inferior iridectomy. Credit: Prof McGhee
Blunt trauma or other ocular disease sequelae associated with diseases such as Marfan’s syndrome and pseudoexfoliation syndrome, affect the integrity of the zonules and can lead to lens subluxation and ultimately dislocation. However, several techniques can address the tendency to lens subluxation at the time of cataract surgery, including the insertion of capsular tension rings and sutured tension segments to artificially stabilise the capsule-intraocular lens (IOL) complex where zonules are compromised2.
References
1. Bassnett, Steven. Zinn’s Zonule. Progress in retinal and eye research. 2021 May; 82:100902. Epub 2020 Sep 25
2: Venkateswaran N, Henderson BA. Loose zonules in cataract surgery. Current Opinion Ophthalmology. 2022 Jan 1; 33(1):53-57

Scott Wilmshurst is a final-year medical student at the University of Auckland (UoA) with an interest in ophthalmology. He recently completed an elective in UoA and Auckland DHB ophthalmology services.

Dr Lize Angelo is an HRC clinical research fellow pursuing a PhD in diagnosing and treating keratoconus, including aspects of equity of access to services in Aotearoa, in the UoA’s ophthalmology department, headed by Professor Charles McGhee.