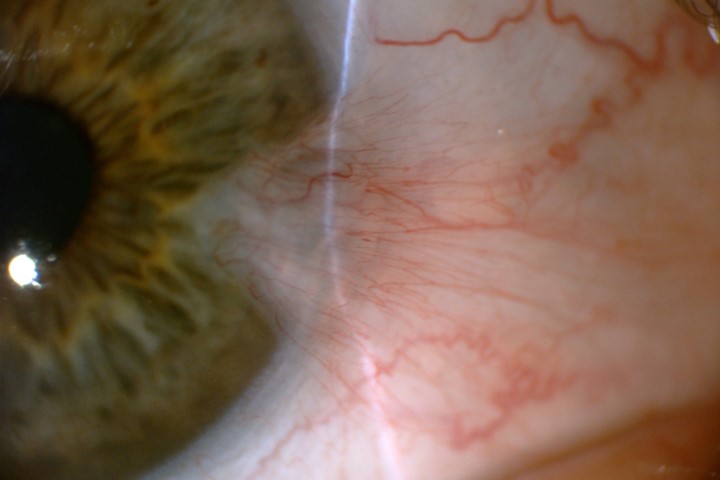
Dry eye disease is a common ocular surface disorder, resulting in one of the most frequently encountered complaints in ophthalmic practice. Whilst the disease is complex and multifactorial, inflammation is a common denominator in DED, which in turn causes further damage to the corneal epithelium and its underlying structures.
Several treatment modalities have been used to suppress inflammation, however, results are variable and the condition can be refractory in some cases. The use of amniotic membrane (AM) as another treatment modality in DED is an exciting clinical development and novel area of research.
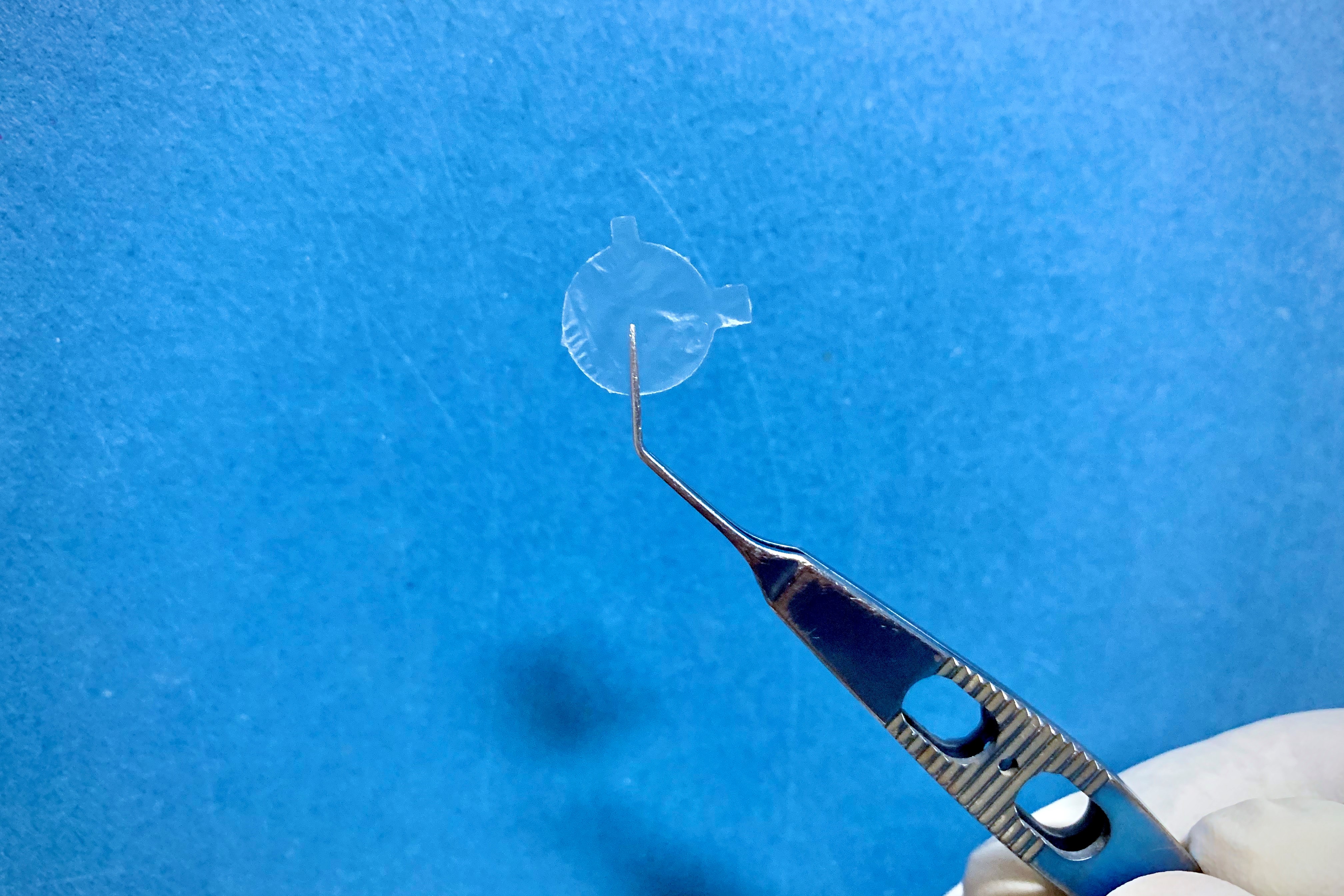
AM is part of the amnion and consists of a single layer of epithelial cells, a basement membrane. Its utility in DED treatment is attributed to its known potent anti-inflammatory properties. AM can either be grafted in theatre with sutures or glue or can be applied in an office setting. There are two types of AM that can be used: cryopreserved or dehydrated. They are proposed for use with specific, typically severe or refractory corneal and conjunctival disorders, including persistent epithelial defect, prevention of ocular complications associated with Stevens- Johnson syndrome and primary or recurrent pterygia. AM can also assist in wound healing and in preventing scar tissue formation as it has powerful antifibrotic and anti-scarring properties but is not typically used as a replacement for bandage contact lens use.
Treatment outcomes in the dry eye amniotic membrane (DREAM) study
McDonald MB, Sheha H, Tighe S et al.
Clin Ophthalmol 2018:12 677–681.
Design: This published study highlights the use of cryopreserved AM in DED. It is a retrospective, multicentre study completed in the USA and has the largest number of recruited cases to date. Patients with refractory DED who received AM and completed at least three months of follow-up were included. Data collected were demographics; medical history, including previous and current ocular treatment; diagnosis; clinical presentations; comorbidity; duration; and frequency of treatment with cryopreserved amniotic membrane and concomitant medications. The primary outcome was the change in the 2007 TFOS Dry Eye Workshop (DEWS) score after treatment.
Outcome: A total of 97 eyes of 84 patients [12 (14%) male, 69 (82%) female, and 3 (4%) unknown] were included in the study. Patients exhibited severe dry eye (DEWS 3.25±0.5) despite maximal medical treatments. AM was applied at the office. The average duration of AM placement was 5.4±2.8 days, with a range of 2–11 days. AM was removed in 4% after two days due to AM intolerance and one AM fell out of the eye after two days. The overall DEWS score was significantly reduced from 3.25±0.5 at the baseline to 1.44±0.6 at one week (p<0.001), 1.45±0.6 at one month (p<0.001) and 1.47±0.6 at three months (p<0.001).
Comment: This study demonstrates the therapeutic benefits of AM in the treatment of DED, which can be attributed to multiple potential mechanisms of action: first, AM acts as a therapeutic bandage that keeps the eye moist by retaining tears and protecting the ocular surface from the surrounding environment; second, it controls ocular surface inflammation. Whilst patient symptoms improved at three months, it remains to be seen if a beneficial effect extends beyond this time.
The authors concluded that AM is a promising treatment for promoting recovery of the ocular surface and reducing signs and symptoms in moderate-to-severe DED.
Efficacy of self-retained cryopreserved amniotic membrane for neuropathic corneal pain
Morkin MI and Hamrah P.
Ocul Surf 2018:16(1): 132–138.
Design: Neuropathic corneal pain (NCP) results from damaged trigeminal nerve terminals, and the diagnosis and treatment of this rare condition is challenging. In this paper, the authors evaluated the efficacy, safety and tolerability of cryopreserved AM (ProKera) in the treatment of this condition.
Outcome: Diagnosis of NCP was made in the presence of confirmed corneal nerve damage by in vivo confocal microscopy (IVCM) with an otherwise normal clinical slit-lamp examination, along with the absence of active ocular surface disease or concomitant causes of pain or comorbidities. AM was applied to 10 eyes of nine patients. Pain severity was found to improve by 72.5±8.4% over the 6.4±1.1 day retention period. Over the average follow-up period of 9.3 ± 0.8 months (range 7.6–13.8 months), only two patients reported recurrence of pain after a mean of 6.0 ± 2.1 months, and this was resolved by further successful treatment with AM.
IVCM showed a 37±18% statistically significant increase in total nerve density, from 17,701±1,316 to 21,891±2,041 μm/ mm2 (p=0.047), while the fellow untreated eye, which acted as a control, did not show a significant change. Best-corrected distance visual acuity pre and post-AM implantation remained statistically unchanged in all eyes immediately after removal and at the final follow-up visit
Comment: The authors concluded that AM provides a safe and effective therapeutic approach to achieving sustained control of pain in patients affected by NCP.
The use of self-retained, cryopreserved amniotic membrane for Sjögren’s syndrome : a case series
Shafer B, Fuerst Ngā mihi, Massaro-Giordano M, et al.
Digit J Ophthalmol. 2019:25(2): 21–25.
Design: This is a short case series of six patients with Sjögren’s syndrome (SS). All patients were female; mean age, 62.5 ± 13.0 years (ranging from 49 to 86 years).
Outcome: There was an improvement in clinical signs in 83% of cases without noticeable changes in visual acuity. Foreign body sensation and blurred vision were reported by 50% during insertion of the AM and one patient was intolerant to the AM. A relapse in symptoms and signs was observed in the five patients who completed the study, within one month of AM removal.
Comment: The author concluded that self-retained cryopreserved- AM implantation has a place in managing SS patients with severe ocular surface disease, refractory to standard treatment. However, the effects were found to be transient. Further, larger studies are needed to confirm these benefits and a cost effectiveness study would provide clinicians with a better understanding of where AM transplantation fits in the already complex treatment paradigm protocol for DED.
Dr Rasha Altaie is a consultant ophthalmologist with Counties Manukau DHB and Milford Eye with specialist knowledge in cornea and anterior segment disease, and an honorary senior lecturer at the University of Auckland.