Friday coffee club, two weeks before Christmas, one club member casually described the recent occurrence of a missing circle of vision, filled-in with a metallic scotoma in the inferotemporal quadrant of his left visual field. This precisely described event was monocular and resolved over five minutes. I knew he had a few health issues and I also noticed that his left pupil was smaller than his right. He has mild myopia with regular astigmatism and normal discs and retina, no headache and no inflammatory symptoms. With permission I phoned Greenlane’s eye department and asked if he could be seen.
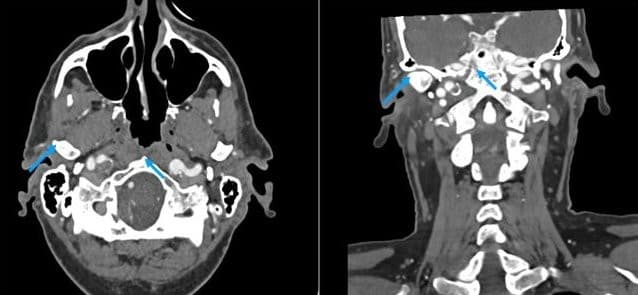
My friend was full of praise for the attention he received. His medical history included treated, systemic hypertension since the age of 30 and takotsubo cardiomyopathy. The conclusion of the eye department team, which included a neurology consult, was that he had suffered a retinal arteriolar embolism that had moved on without causing lasting damage to his retina – the cardiomyopathy being the most likely culprit. He was prescribed blood thinners and an outpatient CT angiogram was arranged to check on the patency of his carotid arteries.
Takotsubo cardiomyopathy is sometimes called ‘broken heart syndrome’. The name ‘takotsubo’ is taken from distinctive Japanese octopus traps, since hearts with takotsubo cardiomyopathy have a similar shape. In most cases, the cardiomyopathy is temporary but in this gentleman’s case the takotsubo cardiomyopathy resulted in a permanent reduction in ejection fraction to 30%, so his heart contracts poorly and only 30% of the blood in the left ventricle is ejected (a normal ejection fraction is between 55 and 70%). In takotsubo, the cause of the myopathy is non-ischaemic (the coronary blood vessels are not narrowed as with most cardiomyopathies); it may occur suddenly after extreme emotional distress and is usually reversible.