







Effects of upper eyelid blepharoplasty on perceived attractiveness, success and health
Sönmez M, Solmaz I, Ertan E
Korean J Ophthalmol. 2024 Aug 16;38(6):437–440
Review: A total of 210 observers (53.2% female) were asked to grade people’s faces online, rating them on attractiveness, perceived success, health and age. The images graded were a mixture of 12 female blepharoplasty patients. Images before and after surgery were interspersed in the review
Observers graded patient age at 51.75 ± 9.78 years preoperatively, which decreased to 42.10 ± 9.34 years post-surgery, which was a statistically significant reduction (p=0.01). Attractiveness, perceived health and success were also graded higher (p=0.01) in the post-surgery group.
Although about 20% of observers had had previous plastic surgery, their grading was no different from those who had not (p=0.01). Observers were blinded to the purpose of the grading.
The noted limitations included the small sample size of photos being graded and photos only being of female patients.
Comment: We know that the periocular area is a significant determinant of perceived ageing, so this study confirms (albeit weakly) that periocular changes can have a measurable impact on perceived age. There are modest effects on perceived success, health and attractiveness, which are mirrored by other studies looking at ptosis etc. Although blepharoplasty is commonly done for functional reasons, there are broader psychosocial impacts that are useful to understand, especially for those requesting cosmetic blepharoplasty.
Chalazion treatment: a concise review of clinical trials
Tashbayev B, Chenb X, Utheim T
Current Eye Research, 49(2), 109–118
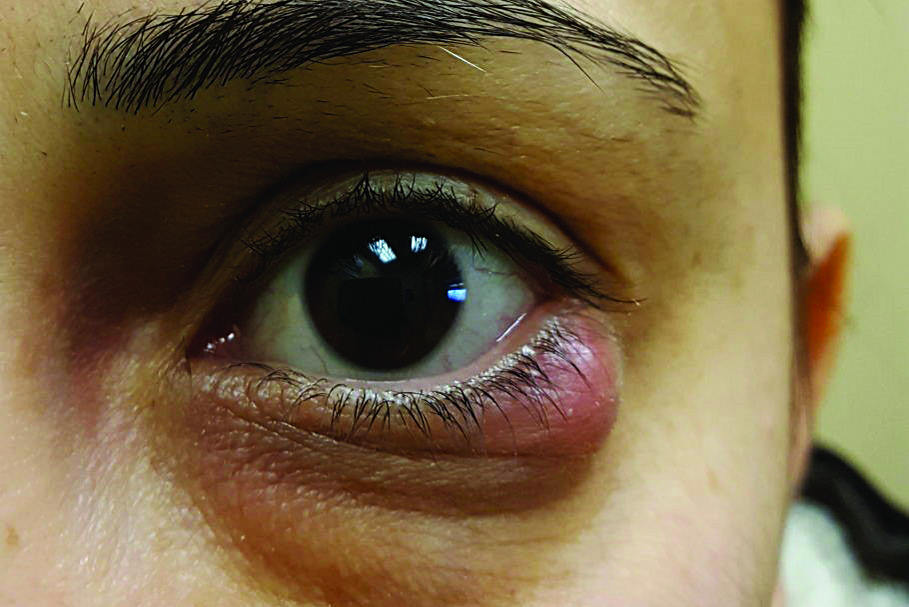
Review: This review of current evidence for chalazion treatment evaluated hot compresses, triamcinolone injection, incision/curettage and other experimental methods.
Findings showed warm compresses and lid care had low resolution rates (~33.8%), even when combined with topical antibiotic/steroid. Intralesional triamcinolone had reasonable resolution rates in small to medium chalazion (70–92%) but was less effective for large chalazion and had some minor side effects, including visible bruising.
Surgery had good success rates (79–100%) and was better for large or refractory lesions. However, it is more invasive and carries the risk of permanent damage to the meibomian glands. There was weak evidence for experimental options such as botox, whose mechanisms are also unknown. Pooled randomised controlled trials showed no difference between triamcinolone and surgery; however, recovery is quicker with surgery, so maybe a combined approach is best for large or difficult cases. Conservative treatment showed the highest recurrence rate (~46%), followed by triamcinolone (~34%) then surgery (~19%).
The study’s limitations include inconsistent outcome measurements and duration of follow-up. There was also minimal evidence with conservative treatment and newer options, such as intense pulsed light, are not as well understood.
Comment: These clinical recommendations support what we see in practice. For small to medium lesions where conservative treatment has failed (no improvement within four to six weeks), intralesional steroid is typically offered. For larger or more recurrent lesions, surgery is first choice. Many people in my practice choose surgery as it can be done on the day and has quicker recovery. However, it is important to understand that surgery is potentially destructive to the meibomian glands so must be judiciously used. Triamcinolone is becoming more common as patients are being referred earlier and there is good general awareness from referrers about treatment options compared to many years ago.
Corneal biophysical changes after upper eyelid blepharoplasty and ptosis surgery: a review
Heidari M, Haydar A, Rajabi M, Rafizadeh S
BMC Ophthalmol 23, 253 (2023)
Review: This comprehensive review analysed 40 articles, one review and one case report on the effects of blepharoplasty and ptosis surgery on corneal biomechanics. Notably, some studies showed no corneal changes post-surgery.
In terms of astigmatism, researchers found blepharoplasty had minimal effect compared to ptosis surgery. Many studies showed central corneal flattening following ptosis repair, with severe ptosis (cornea >4mm over limbus) showing much greater improvement in corneal changes when repaired.
They also found where pre-op astigmatism >1.5D, there were greater improvements post-op. Younger patients seemed to show more change, with changes sometimes taking months to stabilise.
With regard to contrast sensitivity and higher-order aberrations, they confirmed upper eyelid surgery improved higher order aberrations and contrast sensitivity (especially in scotopic conditions). These results persist >3 months and are thought to be due to more light entering the eye and less impact from lashes and redundant skin as well as lid margin.
In patients with dry eye, either surgery can worsen dry eye, although the effects resolve within a few months. Thus, recognition of pre-existing dry eye is important and minimising excision of orbicularis muscle helps.
The review’s limitations include its combination of small case reports and observational studies and the fact it compared different outcomes and durations.
Comment: This is a great summary of what is typically poorly understood. Lid surgery can have visual and refractive impacts. If a patient has visible ptosis or astigmatism >1.5D, please look at their lid position and consider correction of ptosis.
For those with severe ptosis, lid correction should be considered prior to measuring biometry as part of cataract surgery. It is important to recognise that cataract surgery can worsen ptosis, which should be discussed with the patient.
My general rule is: if there is lid skin touching the lashes, or the lid margin is within 2mm of the pupil, that patient is likely to have some reduction in contrast. Please consider referring such patients to your friendly oculoplastic colleagues for assessment, especially if they have visual concerns.

Dr Sid Ogra is a subspecialty trained oculoplastic and cataract surgeon working at Auckland Eye and Manukau SuperClinic. He has a keen interest in functional and cosmetic surgery, as well as vision correction and pterygium surgery, is part of the National Eye Health Network and is an honorary senior lecturer at the University of Auckland where he supervises international fellows and teaches trainees and undergraduate students.















