A recent diagnosis of Parkinson’s disease has added an unexpected dimension to my personal and professional journey. While it brings its own challenges, it has also sharpened my perspective, reinforcing the importance of adaptability, shared care and focusing on what truly matters in patient care. If anything, it has deepened my appreciation for the power of collaboration, resilience and the privilege of continuing to contribute meaningfully to our professions.
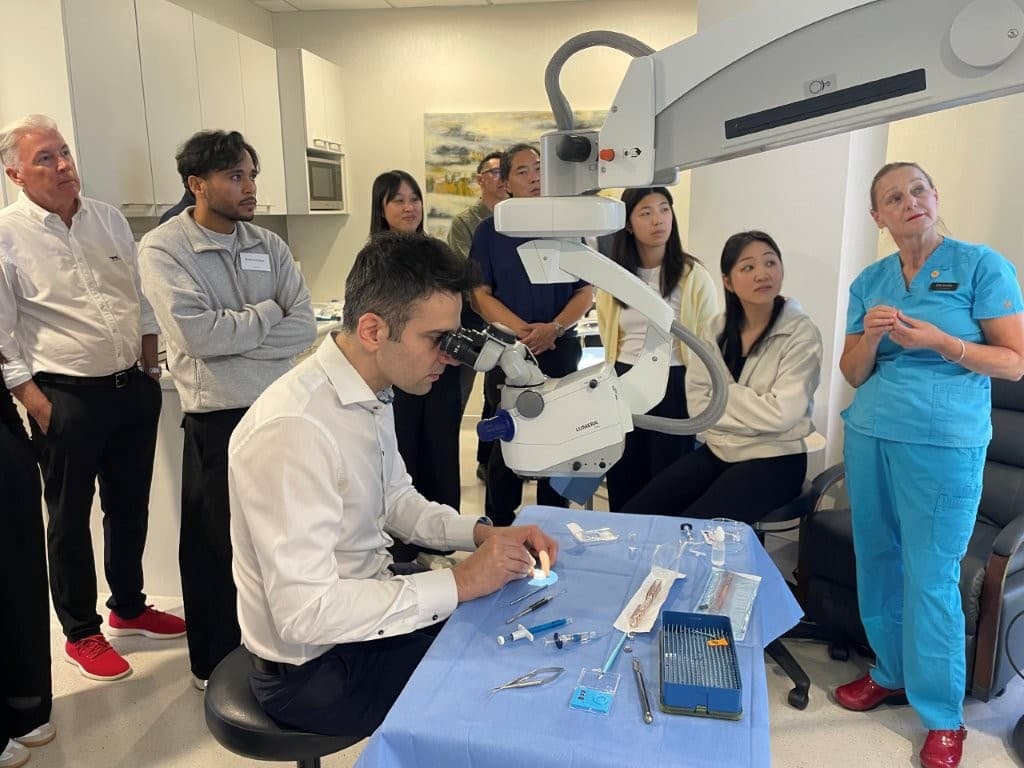
Since stopping cataract and laser surgery, there’s more time for teaching, mentoring and seeing many interesting second opinions for patients from all over the North Island who are struggling with their vision after cataract or laser surgery. It’s also an opportunity to step back and look at the bigger picture of enhancing patient care through closer collaboration between optometry and ophthalmology.
When I began my career in ophthalmology three decades ago, the model of care was largely surgeon-centric. Having received a referral from an optometrist, the ophthalmologist assessed, operated, reviewed, then usually held onto the optometrist’s patient forever. Communication with optometrists certainly occurred, but it was often episodic and letter-based. The ‘episode’ of surgery was the focal point.
Today, the landscape is fundamentally different and unquestionably better.
One of the most significant shifts I have witnessed is the growing recognition of ocular surface disease as a determinant of surgical success. We now understand that a surface-first approach measurably improves refractive accuracy and reduces post-operative dissatisfaction.