In paediatric practice, accuracy in lens power is not only about achieving clear vision, it directly impacts the child’s visual development and their emmetropisation pathway. Unlike adults, where minor prescription discrepancies may result in transient blur or mild discomfort, small errors in a child’s lens power can contribute to abnormal visual feedback, potentially disrupting the cues that guide normal ocular growth.
Refraction (as measured in the consult room) is often considered a fixed universal value, yet this assumption is fundamentally flawed. A prescription is only correct within the exact testing conditions under which it was measured – it is not a context-free value, it reflects the optical correction required only under the test conditions.
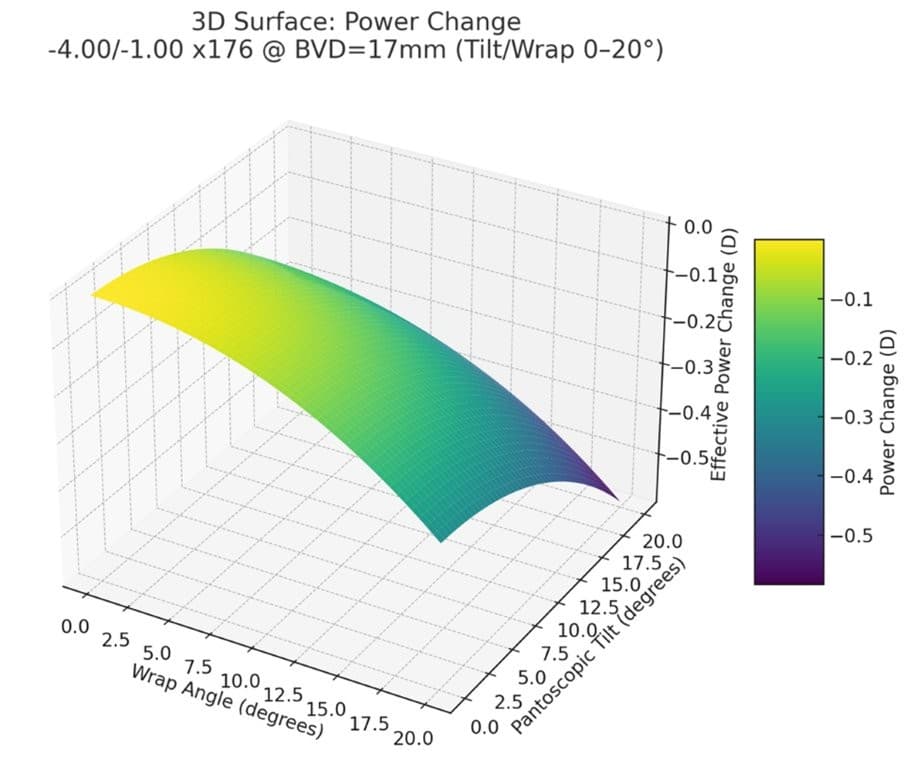
Thus, any change to back vertex distance (BVD), pantoscopic tilt or frame wrap, either in the testing environment or in the final ‘as worn’ spectacles, alters the effective power reaching the retina. Without careful consideration of both the testing and as-worn environment in context, these induced power changes risk inducing either hyperopic or myopic defocus, actively shifting the visual signals that drive eye growth and potentially influencing a child’s ongoing emmetropisation process. This is especially the case with progressive or higher-powered prescriptions (≥ ±4.00 D), although the case for application of precise measurements for every prescription should be readily apparent.